EMT
Respiratory Emergencies
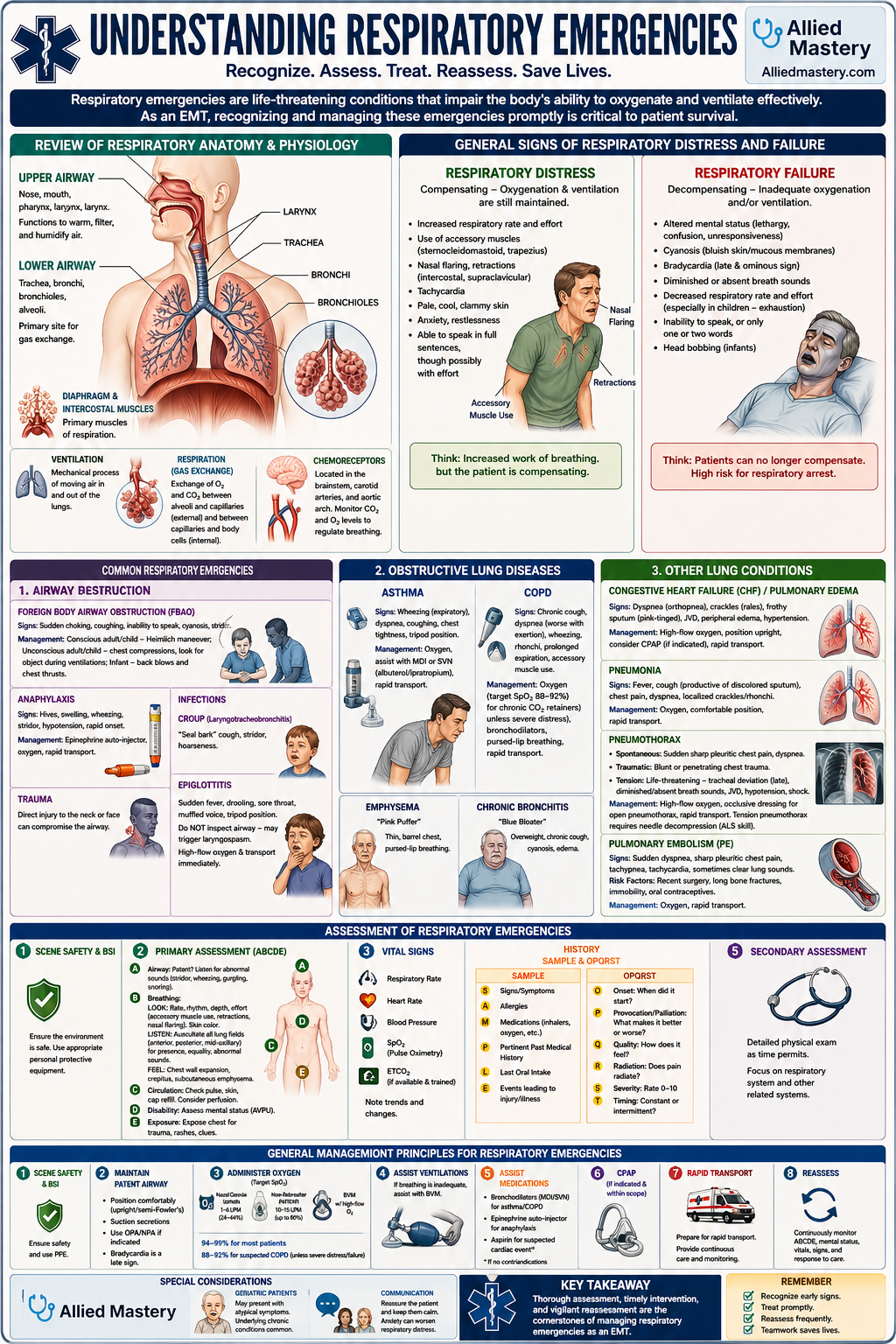
Understanding Respiratory Emergencies
Respiratory emergencies are life-threatening conditions that impair the body's ability to oxygenate and ventilate effectively. As an EMT, recognizing and managing these emergencies promptly is critical to patient survival.
Review of Respiratory Anatomy and Physiology
To understand respiratory emergencies, a brief review of normal respiratory function is essential.
- Upper Airway: Nose, mouth, pharynx, larynx. Functions to warm, filter, and humidify air.
- Lower Airway: Trachea, bronchi, bronchioles, alveoli. The primary site for gas exchange.
- Diaphragm and Intercostal Muscles: Primary muscles of respiration.
- Ventilation: The mechanical process of moving air in and out of the lungs.
- Respiration (Gas Exchange): The physiological process of exchanging oxygen and carbon dioxide between the alveoli and capillaries (external respiration) and between the capillaries and body cells (internal respiration).
- Chemoreceptors: Located in the brainstem, carotid arteries, and aortic arch, they monitor CO2 and O2 levels to regulate breathing.
General Signs of Respiratory Distress and Failure
Respiratory Distress occurs when the patient has difficulty breathing, but their compensatory mechanisms are still maintaining adequate oxygenation and ventilation.
- Increased respiratory rate and effort.
- Use of accessory muscles (sternocleidomastoid, trapezius).
- Nasal flaring, retractions (intercostal, supraclavicular).
- Tachycardia.
- Pale, cool, clammy skin.
- Anxiety, restlessness.
- Able to speak in full sentences, though possibly with effort.
Respiratory Failure occurs when the patient's compensatory mechanisms begin to fail, leading to inadequate oxygenation and/or ventilation.
- Altered mental status (lethargy, confusion, unresponsiveness).
- Cyanosis (bluish discoloration of skin/mucous membranes).
- Bradycardia (a late and ominous sign).
- Diminished or absent breath sounds.
- Decreased respiratory rate and effort (especially in children, indicates exhaustion).
- Inability to speak, or only speaking one or two words.
- Head bobbing (infants).
Common Respiratory Emergencies
1. Airway Obstruction
- Foreign Body Airway Obstruction (FBAO): Complete or partial blockage of the airway by a foreign object.
- Signs: Sudden onset of choking, coughing, inability to speak, cyanosis, stridor.
- Management: Conscious adult/child - Heimlich maneuver; Unconscious adult/child - chest compressions, look for object during ventilations; Infant - back blows and chest thrusts.
- Anaphylaxis: Severe allergic reaction causing swelling of the airway (angioedema).
- Signs: Hives, swelling, wheezing, stridor, hypotension, rapid onset.
- Management: Epinephrine auto-injector, oxygen, rapid transport.
- Trauma: Direct injury to the neck or face can compromise the airway.
- Infections:
- Croup (Laryngotracheobronchitis): Viral infection in children causing swelling of the upper airway. Presents with a "seal bark" cough, stridor, and hoarseness.
- Epiglottitis: Bacterial infection of the epiglottis, a severe medical emergency. Presents with sudden onset of high fever, drooling, sore throat, muffled voice, and tripod position. Do NOT inspect the airway as this can trigger laryngospasm. Provide high-flow oxygen and transport immediately.
2. Obstructive Lung Diseases
- Asthma: Chronic inflammatory disease of the airways causing bronchospasm, increased mucus production, and airway edema, leading to reversible airway obstruction.
- Signs: Wheezing (primarily expiratory), dyspnea, coughing, chest tightness, tripod position.
- Management: Administer oxygen, assist with prescribed metered-dose inhaler (MDI) or small-volume nebulizer (SVN) with albuterol/ipratropium, rapid transport.
- Chronic Obstructive Pulmonary Disease (COPD): A group of progressive lung diseases (emphysema and chronic bronchitis) characterized by irreversible airway obstruction.
- Emphysema: Destruction of alveolar walls, leading to decreased surface area for gas exchange. Often presents with a thin, barrel-chested appearance and pursed-lip breathing ("pink puffer").
- Chronic Bronchitis: Inflammation and excess mucus production in the bronchioles. Often presents with overweight appearance, chronic cough, and cyanosis ("blue bloater").
- Signs: Chronic cough, dyspnea (worsens with exertion), wheezing, rhonchi, prolonged expiration, accessory muscle use.
- Management: Administer oxygen (titrate carefully, maintaining SpO2 88-92% for chronic CO2 retainers unless severe distress), assist with bronchodilators, encourage pursed-lip breathing, rapid transport.
3. Other Lung Conditions
- Congestive Heart Failure (CHF) / Pulmonary Edema: The heart's inability to pump effectively leads to fluid buildup in the lungs (pulmonary edema).
- Signs: Dyspnea (especially while lying down - orthopnea), crackles (rales), frothy sputum (pink-tinged), JVD, peripheral edema, hypertension.
- Management: High-flow oxygen, position upright, consider CPAP (if indicated and within scope), rapid transport.
- Pneumonia: Infection of the lungs, causing inflammation and fluid in the alveoli.
- Signs: Fever, cough (productive of discolored sputum), chest pain, dyspnea, localized crackles/rhonchi.
- Management: Oxygen, comfortable position, rapid transport.
- Pneumothorax: Collapsed lung due to air accumulating in the pleural space.
- Spontaneous Pneumothorax: Often occurs in tall, thin males or those with underlying lung disease. Sudden onset of sharp pleuritic chest pain and dyspnea.
- Traumatic Pneumothorax: Caused by blunt or penetrating trauma to the chest.
- Tension Pneumothorax: Life-threatening. Air enters the pleural space but cannot exit, causing increased pressure that compresses the lung, heart, and great vessels. Leads to tracheal deviation (late sign), diminished/absent breath sounds on affected side, JVD, hypotension, and shock.
- Management: High-flow oxygen, consider occlusive dressing for open pneumothorax, rapid transport. A tension pneumothorax requires needle decompression, which is typically an ALS skill.
- Pulmonary Embolism (PE): Blockage of a pulmonary artery by a blood clot, fat, or air.
- Signs: Sudden onset of dyspnea, sharp pleuritic chest pain, tachypnea, tachycardia, sometimes clear lung sounds. Risk factors include recent surgery, long bone fractures, immobility, oral contraceptives.
- Management: Oxygen, rapid transport.
Assessment of Respiratory Emergencies
- Scene Safety and BSI: Ensure the environment is safe and put on appropriate personal protective equipment.
- Primary Assessment (ABCDE): Focus on immediate life threats.
- Airway: Is it patent? Listen for abnormal sounds (stridor, wheezing, gurgling, snoring).
- Breathing:
- Look: Rate, rhythm, depth, effort (accessory muscle use, retractions, nasal flaring). Skin color (cyanosis, pallor).
- Listen: Auscultate breath sounds in all lung fields (anterior, posterior, mid-axillary) for presence, equality, and abnormal sounds (wheezing, crackles, rhonchi, diminished/absent sounds).
- Feel: Chest wall expansion, crepitus, subcutaneous emphysema.
- Circulation: Assess pulse, skin signs, and cap refill. Consider perfusion status.
- Disability: Assess mental status using AVPU.
- Exposure: Fully expose the chest to assess for trauma, rashes, or other clues.
- Vital Signs: Obtain respiratory rate, heart rate, blood pressure, SpO2, and ETCO2 (if available and trained). Note trends.
- History (SAMPLE and OPQRST for dyspnea/chest pain):
- Signs/Symptoms: What are they experiencing?
- Allergies: Any relevant allergies?
- Medications: What medications do they take (especially inhalers, oxygen)?
- Pertinent past medical history: Asthma, COPD, CHF, recent surgeries, DVT history?
- Last oral intake: Important if intubation might be needed.
- Events leading to injury/illness: What were they doing?
- Onset: When did the dyspnea start?
- Provocation/Palliation: What makes it better or worse?
- Quality: How does it feel (tight, heavy, suffocating)?
- Radiation: Does any pain or discomfort radiate?
- Severity: Rate dyspnea/pain on a 0-10 scale.
- Timing: Is it constant, intermittent?
- Secondary Assessment: Detailed physical exam as time permits, focusing on respiratory system and other related systems.
General Management Principles for Respiratory Emergencies
- Ensure Scene Safety and BSI.
- Maintain a Patent Airway:
- Position the patient comfortably (often upright or semi-Fowler's).
- Suction any secretions, blood, or vomit.
- Use airway adjuncts (OPA/NPA) if indicated and tolerated.
- Administer Oxygen:
- Use appropriate device based on patient's condition and SpO2 target.
- Nasal Cannula: 1-6 LPM (24-44% O2) for mild distress or to maintain SpO2.
- Non-Rebreather Mask: 10-15 LPM (up to 90% O2) for moderate to severe distress.
- Bag-Valve-Mask (BVM): For inadequate breathing or respiratory arrest, connected to high-flow oxygen.
- Target SpO2: Generally 94-99% for most patients. For patients with suspected COPD exacerbation, target 88-92% to avoid suppressing respiratory drive, unless they are in severe distress/failure.
- Assist Ventilations: If breathing is inadequate (too slow, too fast, too shallow), assist with a BVM.
- Assist with Medications (EMT Scope):
- Bronchodilators (e.g., Albuterol, Ipratropium): Administer via MDI or SVN for bronchospasm (asthma, COPD). Ensure patient cooperation and proper technique.
- Epinephrine (auto-injector): For severe anaphylaxis with respiratory compromise. Follow local protocols.
- Aspirin: Consider for dyspnea associated with suspected cardiac event (if no contraindications).
- Continuous Positive Airway Pressure (CPAP): If within scope and indicated for pulmonary edema, COPD exacerbation, or severe asthma. Requires specific training and protocols.
- Rapid Transport: Many respiratory emergencies require advanced care and definitive treatment at a hospital. Prepare for rapid transport and constant reassessment.
- Reassessment: Continuously monitor the patient's airway, breathing, circulation, mental status, and vital signs. Note response to interventions.
Special Considerations
- Pediatric Patients: Children compensate longer but decompensate rapidly. Look for retractions, nasal flaring, head bobbing, and grunting. Bradycardia is a pre-terminal sign of hypoxia.
- Geriatric Patients: May present with atypical symptoms. Underlying chronic conditions (CHF, COPD) are common. Decreased physiological reserves.
- Communication: Reassure the patient and keep them calm, as anxiety can worsen respiratory distress.
Thorough assessment, timely intervention, and vigilant reassessment are the cornerstones of managing respiratory emergencies as an EMT.
Ready to Go Deeper?
This is just a sample of what Allied Mastery offers. Sign up to unlock our full library, create custom quizzes, track your performance, and more.