MA
Patient Intake and Vital Signs
Patient Intake
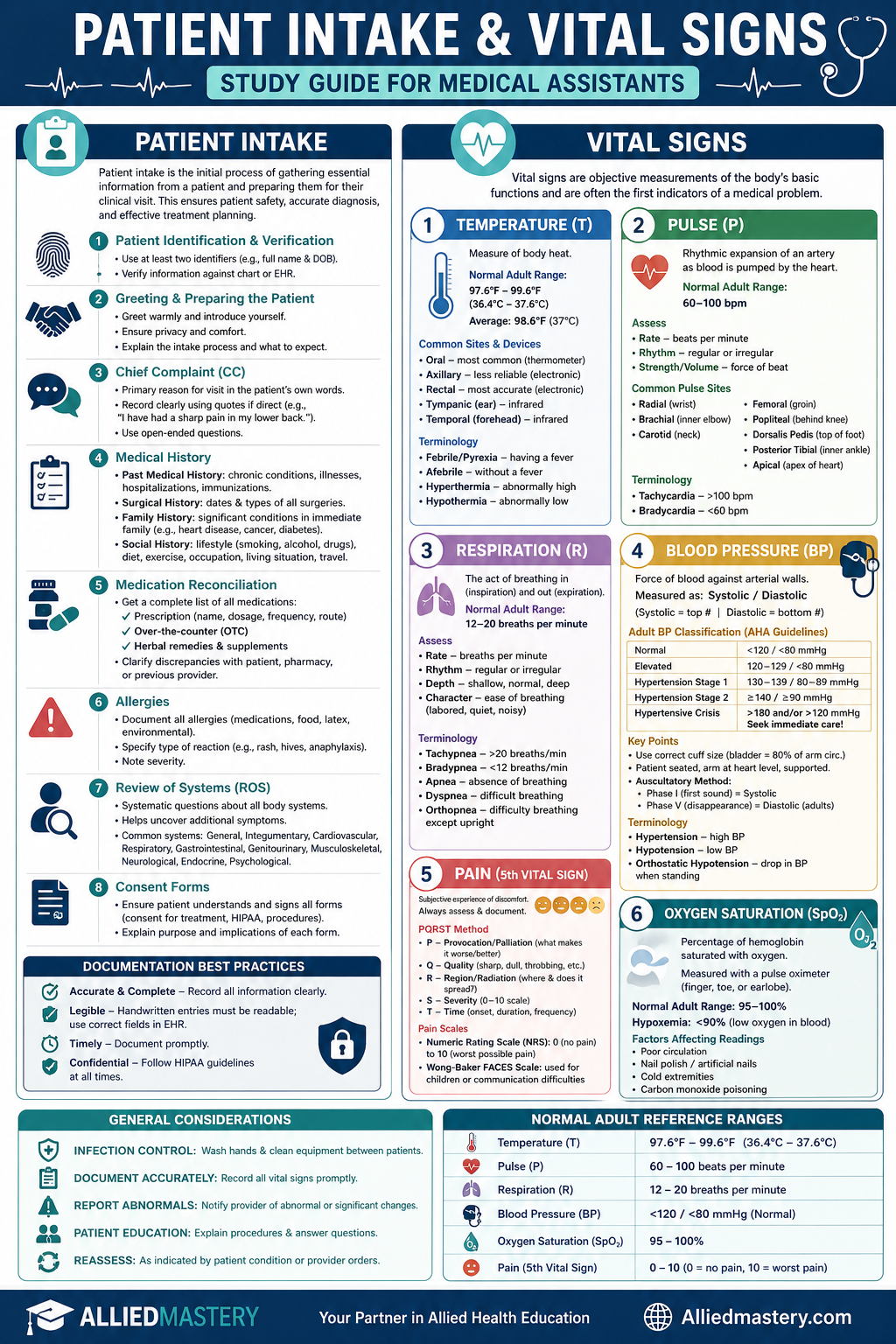
Patient intake is the initial process of gathering essential information from a patient and preparing them for their clinical visit. This crucial step ensures patient safety, facilitates accurate diagnosis, and supports effective treatment planning.
Key Components of Patient Intake
1. Patient Identification and Verification
- Two Identifiers: Always use at least two forms of identification (e.g., full name and date of birth) to ensure you are treating the correct patient. This is a critical safety protocol.
- Cross-referencing: Verify information against the patient's chart or electronic health record (EHR).
2. Greeting and Preparing the Patient
- Professionalism: Greet the patient warmly and professionally, introducing yourself and explaining your role.
- Privacy: Ensure the patient's privacy and comfort during the intake process.
- Explanation: Briefly explain the intake process and what to expect during their visit.
3. Chief Complaint (CC)
- Definition: The primary reason for the patient's visit, stated in their own words.
- Documentation: Record the CC clearly and concisely, using quotation marks if directly quoting the patient (e.g., "I have had a sharp pain in my lower back for two days.").
- Open-ended Questions: Encourage the patient to elaborate without leading them.
4. Medical History
- Past Medical History (PMH):
- Chronic conditions (e.g., diabetes, hypertension, asthma)
- Previous illnesses and hospitalizations
- Immunization status
- Surgical History (PSH): Dates and types of all previous surgeries.
- Family History (FH): Significant medical conditions in immediate family members (parents, siblings, children) that may have a genetic component (e.g., heart disease, cancer, diabetes).
- Social History (SH):
- Lifestyle factors (e.g., smoking, alcohol use, recreational drug use)
- Diet and exercise habits
- Occupation and living situation
- Travel history
5. Medication Reconciliation
- Comprehensive List: Obtain a complete and accurate list of all medications the patient is currently taking, including:
- Prescription medications (name, dosage, frequency, route)
- Over-the-counter (OTC) medications
- Herbal remedies and supplements
- Verification: Clarify any discrepancies or unknown medications with the patient and, if necessary, with their pharmacy or previous provider.
6. Allergies
- Type of Reaction: Document all known allergies, including medications, food, latex, and environmental allergens.
- Severity: Crucially, specify the type of reaction the patient experiences (e.g., rash, hives, anaphylaxis).
7. Review of Systems (ROS)
- Systematic Inquiry: A series of questions about all body systems to identify any current or past symptoms that the patient may not have mentioned as part of their chief complaint. This helps uncover additional problems.
- Organized Approach: Typically reviewed system by system (e.g., general, integumentary, cardiovascular, respiratory, gastrointestinal, genitourinary, musculoskeletal, neurological, endocrine, psychological).
8. Consent Forms
- Informed Consent: Ensure the patient understands and signs all necessary consent forms, such as consent for treatment, privacy practices (HIPAA), and any specific procedures.
- Patient Education: Explain the purpose and implications of each form clearly.
Documentation
- Accuracy and Completeness: All collected information must be documented accurately, clearly, concisely, and completely in the patient's medical record.
- Legibility: If handwritten, ensure legibility. In EHRs, use correct fields.
- Timeliness: Document information promptly to maintain an up-to-date record.
- HIPAA Compliance: Maintain patient confidentiality at all times.
Vital Signs
Vital signs are objective measurements of the body's most basic functions, providing critical information about a patient's physiological status and indicating their overall health. They are often the first indicators of a medical problem.
The Cardinal Vital Signs
1. Temperature (T)
- Definition: A measure of the body's heat production and heat loss.
- Normal Adult Range: 97.6°F to 99.6°F (36.4°C to 37.6°C). A common average is 98.6°F (37°C).
- Factors Affecting Temperature: Infection, inflammation, exercise, time of day, age, environmental temperature, hormonal changes.
- Measurement Sites and Devices:
- Oral: Most common, reliable. Not suitable for unconscious, uncooperative, or young children. (Thermometer: glass, electronic)
- Axillary (Armpit): Less reliable, often lower than oral. Used when oral/rectal are contraindicated. (Electronic thermometer)
- Rectal: Most accurate, invasive. Used for infants, young children, or when other sites are impractical. (Electronic thermometer, designated for rectal use)
- Tympanic (Ear): Measures infrared heat from the eardrum. Quick, non-invasive. (Tympanic thermometer)
- Temporal (Forehead): Measures infrared heat from the temporal artery. Quick, non-invasive. (Temporal artery thermometer)
- Terminology:
- Febrile/Pyrexia: Having a fever.
- Afebrile: Without a fever.
- Hyperthermia: Abnormally high body temperature.
- Hypothermia: Abnormally low body temperature.
2. Pulse (P)
- Definition: The rhythmic expansion and contraction of an artery as blood is pumped through it by the heart.
- Normal Adult Range: 60-100 beats per minute (bpm).
- Factors Affecting Pulse: Exercise, stress, fever, medications, hemorrhage, heart disease.
- Characteristics to Assess:
- Rate: Number of beats per minute.
- Rhythm: Regularity of beats (regular, irregular).
- Strength/Volume: Force of the beat (strong, bounding, weak, thready).
- Common Pulse Sites:
- Radial: Thumb side of the wrist (most common).
- Brachial: Inner aspect of the elbow (used for blood pressure, infants).
- Carotid: Side of the neck (used during CPR for adults).
- Femoral: Groin area.
- Popliteal: Behind the knee.
- Dorsalis Pedis: Top of the foot.
- Posterior Tibial: Inner ankle.
- Apical: Apex of the heart, listened to with a stethoscope (most accurate, used for infants, patients with irregular rhythms).
- Terminology:
- Tachycardia: Pulse rate over 100 bpm.
- Bradycardia: Pulse rate under 60 bpm.
3. Respiration (R)
- Definition: The act of breathing, involving both inspiration (inhalation) and expiration (exhalation).
- Normal Adult Range: 12-20 breaths per minute.
- Factors Affecting Respiration: Exercise, anxiety, pain, medications, lung disease, fever.
- Characteristics to Assess (Observe discreetly, often while taking pulse):
- Rate: Number of breaths per minute.
- Rhythm: Regularity of breathing pattern.
- Depth: Amount of air exchanged (shallow, normal, deep).
- Character: Ease of breathing (labored, quiet, noisy).
- Terminology:
- Tachypnea: Respiration rate over 20 breaths per minute.
- Bradypnea: Respiration rate under 12 breaths per minute.
- Apnea: Absence of breathing.
- Dyspnea: Difficult or labored breathing.
- Orthopnea: Difficulty breathing except in an upright position.
4. Blood Pressure (BP)
- Definition: The force exerted by the blood against the arterial walls during the cardiac cycle.
- Measurement: Expressed as a fraction: Systolic Pressure / Diastolic Pressure.
- Systolic: Maximum pressure during ventricular contraction (ejection of blood).
- Diastolic: Minimum pressure during ventricular relaxation (heart at rest).
- Normal Adult Range (AHA Guidelines):
- Normal: Systolic <120 mmHg AND Diastolic <80 mmHg
- Elevated: Systolic 120-129 mmHg AND Diastolic <80 mmHg
- Hypertension Stage 1: Systolic 130-139 mmHg OR Diastolic 80-89 mmHg
- Hypertension Stage 2: Systolic ≥140 mmHg OR Diastolic ≥90 mmHg
- Hypertensive Crisis: Systolic >180 mmHg AND/OR Diastolic >120 mmHg (seek immediate medical attention)
- Equipment:
- Sphygmomanometer: Consists of a cuff, inflation bulb, and manometer (aneroid or mercury).
- Stethoscope: Used to auscultate Korotkoff sounds.
- Technique:
- Patient Position: Seated, feet flat on floor, arm supported at heart level, relaxed.
- Cuff Size: Crucial for accuracy. Bladder should encircle 80% of arm circumference.
- Palpatory Method: Palpate radial pulse, inflate cuff until pulse disappears, note pressure, then deflate. Add 30 mmHg to this value for auscultatory measurement to avoid an auscultatory gap.
- Auscultatory Method: Place stethoscope over brachial artery. Inflate cuff to palpatory level. Slowly deflate cuff (2-3 mmHg/sec) while listening for Korotkoff sounds:
- Phase I: First clear, tapping sound (Systolic BP).
- Phase V: Disappearance of sounds (Diastolic BP for adults).
- Factors Affecting BP: Age, sex, race, exercise, stress, medications, disease processes, cuff size, arm position.
- Terminology:
- Hypertension: High blood pressure.
- Hypotension: Low blood pressure.
- Orthostatic Hypotension: A drop in BP when changing from lying to sitting or standing.
5. Pain (The 5th Vital Sign)
- Definition: An unpleasant sensory and emotional experience associated with actual or potential tissue damage. It is subjective.
- Assessment: Always ask the patient about pain.
- Location: Where is the pain?
- Intensity: On a scale of 0-10 (0=no pain, 10=worst possible pain).
- Quality: What does it feel like? (e.g., sharp, dull, throbbing, burning)
- Onset/Duration: When did it start? How long does it last?
- Aggravating/Alleviating Factors: What makes it worse/better?
- Impact: How does it affect daily activities?
- Pain Scales:
- Numeric Rating Scale (NRS): 0-10 for adults and older children.
- Wong-Baker FACES Pain Rating Scale: Uses faces to express pain levels, suitable for children or those with communication difficulties.
6. Oxygen Saturation (SpO2)
- Definition: The percentage of hemoglobin saturated with oxygen in arterial blood.
- Measurement: Non-invasively measured with a pulse oximeter, typically placed on a finger, toe, or earlobe.
- Normal Adult Range: 95-100% on room air.
- Hypoxemia: Oxygen saturation below 90% (indicates low oxygen in blood).
- Factors Affecting Readings: Poor circulation, nail polish, artificial nails, cold extremities, carbon monoxide poisoning.
General Considerations for Vital Signs
- Infection Control: Always practice proper hand hygiene before and after taking vital signs. Clean equipment (e.g., stethoscope, blood pressure cuff) between patients.
- Documentation: Record all vital signs accurately and promptly in the patient's chart or EHR.
- Reporting Abnormalities: Immediately report any abnormal or significant changes in vital signs to the physician or supervising nurse.
- Patient Education: Explain the purpose of vital sign measurement to the patient and answer any questions they may have.
- Reassessment: Reassess vital signs as indicated by the patient's condition or physician's orders.
By mastering patient intake and vital sign assessment, medical assistants provide critical support in patient care, contributing to accurate diagnosis and effective treatment.
Ready to Go Deeper?
This is just a sample of what Allied Mastery offers. Sign up to unlock our full library, create custom quizzes, track your performance, and more.